Diagnosis
Diagnosis
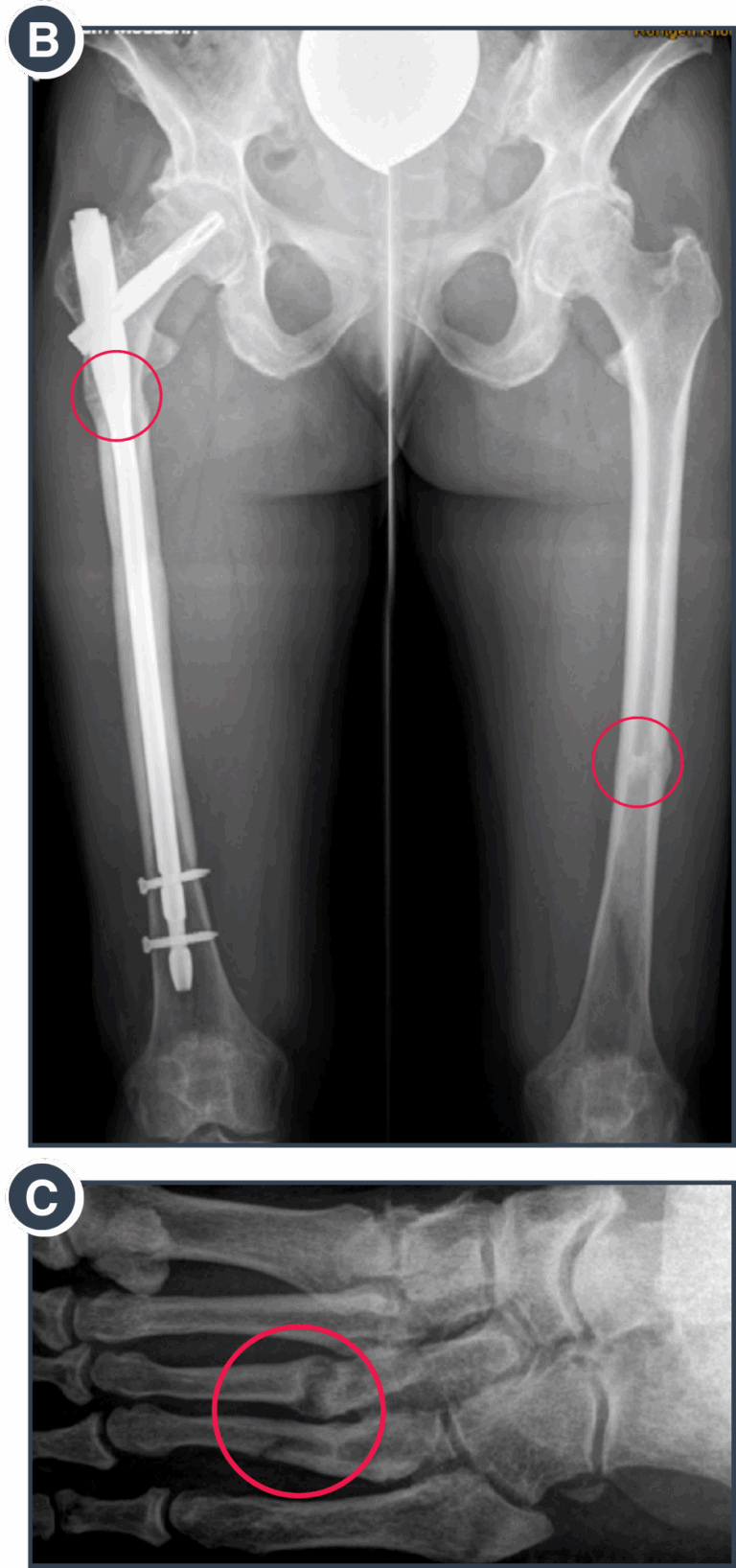
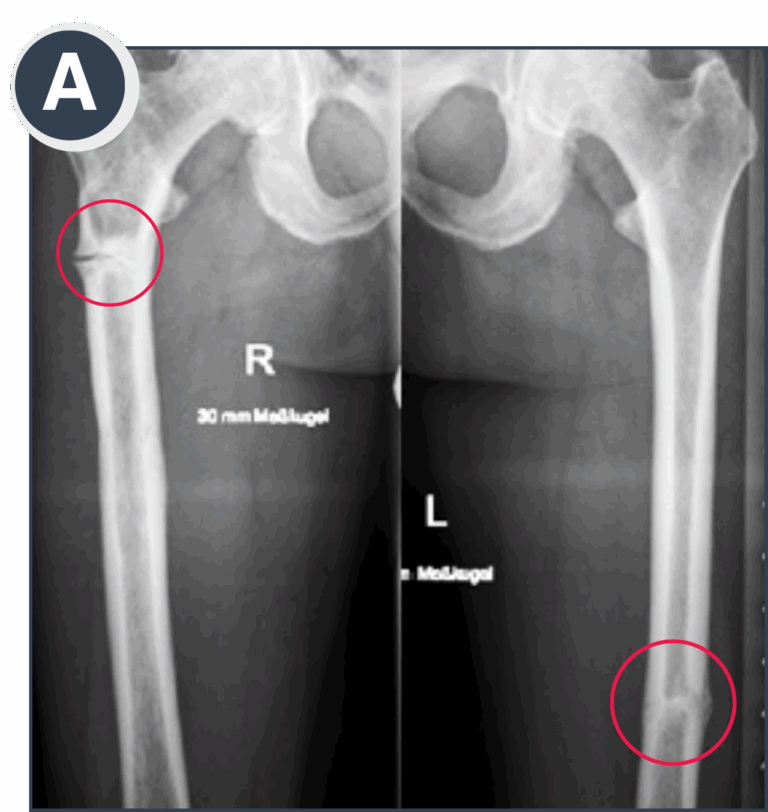
An accurate diagnosis is important for determining the optimal treatment strategy. Because HPP affects every person differently, symptoms and complications from the condition that require medical and/or surgical treatment need to be evaluated on a case-by-case basis. However, some common complications often occur within specific areas of the body. For example, bone-related complications such as fractures, pseudo-fractures, and bone bruises, typically affect the bones of the lower extremities, specifically the femur, tibia, and metatarsal bones. And, bone marrow lesions resulting from injury – or more frequently from repetitive strain in the context of everyday activities – are typically seen in short bones (those that are approximately equal in length, width, and thickness) or in those parts of long bones (those that are longer than they are wide) that are close to the joints.
In contrast, (pseudo-) fractures due to HPP typically occur along the axis (diaphysis) of long bones. Early signs of bone marrow lesions can be detected by magnetic resonance imaging (MRI) before visible damage can be seen on conventional X-ray exams. In case of a suspected diaphyseal (pseudo-) fracture, thorough assessment of conventional x-ray imaging is essential and, in many instances, more meaningful than CT or MRI. Ambiguous findings should be addressed by a bone scan. CT and/or MRI are not mandatory, but may be helpful for specific questions regarding treatment strategy. If a pseudo-fracture is diagnosed, mindful clinical—and in case of doubt, radiographic assessment—is warranted.
 Treatment & Management
Treatment & Management
Non Surgical Treatment:
To compensate for or correct a skeletal irregularity, conservative options, including physiotherapy and braces, should be considered prior to surgery. Particularly with younger patients, medical treatment to compensate for metabolic deficits may also help to correct skeletal irregularities during growth ¹. Early-stage bone marrow lesions should be treated conservatively with suspended weight bearing strictly below the patient’s threshold of pain to allow the bone to heal, and frequently seen concurrent Vitamin D deficiency should also be compensated for mindfully.
Acknowledging that the healing process will take longer for patients with HPP than for those without it, more invasive treatments may not be needed if a patient consequently adheres to this treatment. For pseudo-fractures, suspended weight bearing should be recommended to prevent fracture completion. Although spontaneous bone healing over long periods of time has been seen in some cases and there is some evidence to support treatment with teriparatide, the latter has not been approved for that indication.
Furthermore, despite these treatment considerations, the risk of fracture progression is high. Therefore, in many cases, surgery is advisable to regain mobility and prevent complete fractures or potential deformities. Enzyme replacement therapy (ERT ) has been shown to promote bone healing, even for long-standing pseudofractures, and may even prevent the need for surgery in certain settings ². Currently, the combination of ERT with appropriate surgery appears to offer the best results for patients.