
 What is Hypophosphatasia?
What is Hypophosphatasia?
 Diverse Experiences, United Community
Diverse Experiences, United Community
 Lindsey’s story
Lindsey’s story
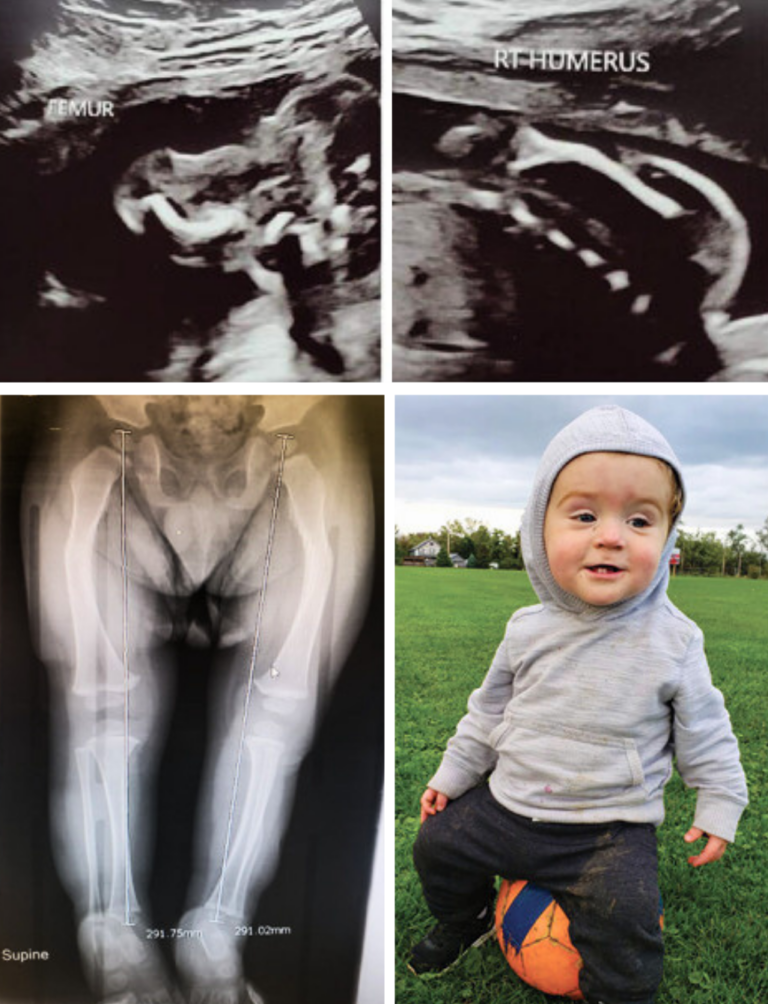
“During my 12-week ultrasound, I could see the expression leave the technician’s face. They couldn’t see our baby’s hands, feet or the middle part of her face. We were sent to a perinatologist who said the baby had some sort of skeletal dysplasia. At 20 weeks, another specialist said that our baby had osteogenesis imperfecta and that she would likely die shortly after birth if she survived delivery. We held strong to our faith and kept moving forward. While we tried to remain hopeful – setting up a crib, we also planned for the worst – making funeral arrangements.
At 37 weeks, Evie was born with short stature and raspy breathing, but she made it. We soaked up every minute of that first night not knowing how much time we would have and were in disbelief when, the next day, we were told we could take her home. Two weeks later, we were back in the hospital when she started having seizures and this time, we got the HPP diagnosis.
We now had a path to a clinical trial and treatment, but we never really knew what was coming next. Over the years, Evie has endured a short time on a ventilator, months on oxygen support, seizures, craniosynostosis, a dozen surgeries and more, all of which was uncharted territory in 2010. Because we expected to have no time with her at all, every moment felt like such a gift.

Amy’s story
“At my 20-week ultrasound, I was told ‘something is wrong’ and in an instant, my dreams for the pregnancy and my baby’s life were shattered. Specialists said my baby could have HPP or osteogenesis imperfecta, but when she was born – she seemed healthy – so I breathed a sigh of relief. With no time in the NICU and only a few days in the hospital, we headed home. But within a few days, everything changed. One morning, Aubrey seemed stiff and almost frozen. The local hospital did rounds of tests and found nothing. The next day it happened again and this time, I wasn’t leaving the hospital without answers. We eventually found our way to a children’s hospital where Aubrey was diagnosed with HPP and soon after, was enrolled in a clinical trial and started treatment.
That was more than 8 years ago. Since that time, Aubrey has had more than a dozen surgeries, endless hospital visits and weekly physical and feeding therapy. But HPP doesn’t define her. She is full of personality (including a very sassy attitude), makes friends with everyone and is exceptionally smart for her age.
Our life as a family is about managing appointments for HPP, but it’s also about what other families have to deal with – two working parents, two children in school (Aubrey has a younger sibling) and normal everyday challenges. I realize now that I have new, different dreams for my daughter and for my family, but dreams nonetheless.”
– Amy Britt, mother of Aubrey

Laiken’s story
“At 24 weeks pregnant, we received the HPP diagnosis for our baby. My pregnancy joy vanished as every appointment seemed filled with constant reminders that I could either lose my baby at birth or have a child with severe medical complexities. It was extremely overwhelming, scary and isolating. When I think back on the day I gave birth, I still get emotional as that was the moment we would find out if he would live or die.
Rowan did live and to us, he is perfect. At 14 months old, he is shorter than average and has vitamin deficiencies, but his developmental motor skills are on track and he is doing really well. We have regular treatment injections, supplements and therapy, but otherwise, our daily life is like any other family.
What is different is what we have learned throughout this journey. Rowan has taught us so much — to not focus on the ‘what ifs,’ to take one step at a time and to enjoy every moment. He is truly the greatest blessing to our family.”
– Laiken Latimer, mother of Rowan

 Commonly Asked Questions
Commonly Asked Questions
 What can I expect with HPP?
What can I expect with HPP?
HPP presents with a remarkably broad range of severity in patients. Your child’s story will undoubtedly be very different from others, even among affected members of the same family. Some children have severe complications early in life, whereas others have less severe disease that may cause problems during childhood but can improve during puberty and young adulthood. It can be a challenging disease in which you need to expect the unexpected, but there are also many moments of joy and happiness as with the arrival of any baby.
 Will my baby survive?
Will my baby survive?
HPP can be a life-threatening disease and there are cases where pregnancies end in stillbirth or affected newborns survive only for a few days. That said, many babies not only survive, but thrive. Good neonatal care with an expert team that understands HPP is essential. Treatment with Strensiq® (asfotase alfa), when indicated, has led to significant improvements in survival and importantly, in meaningful survival without respiratory support. Additionally, significant improvements in motor development, growth and skeletal mineralization can occur with the use of Strensiq® when needed.
 What doctors do I need to talk to?
What doctors do I need to talk to?
The healthcare professionals will vary depending on the severity of your baby’s HPP. What is key is having a multi-disciplinary approach – a team of doctors from different specialties and other disciplines that work together to provide the best care possible for your child. While pregnant, the core care team typically includes the obstetrician, a maternal-fetal medicine specialist, a metabolic bone specialist (who is often a pediatric endocrinologist or geneticist), and a genetic counselor. Once the baby is born, the core care team often includes a neonatologist, a metabolic bone specialist and a genetic counselor. Depending on the problems your baby may be experiencing, a child neurologist, a pulmonologist, a gastroenterologist, a pediatric neurosurgeon, a pediatric orthopedic surgeon, a chronic ventilator team, and a dietician may be needed for care.
 What kind of therapy/treatment do I need ready
What kind of therapy/treatment do I need ready
before the baby is born (or soon after)?
The kind of treatments that your child will need depends on the severity of HPP. One of the most important things to do is to reach out to Soft Bones as soon as you have the HPP diagnosis to ensure that your hospital will have access to Strensiq® (asfotase alfa), should it be needed. Time is of the essence for newborns needing medication so it is critical this is set up in advance.
If your infant has the perinatal form of HPP, they may require assistance with breathing. Your child may also likely need a specialized medical team and assistance with feeding. If your child does not have the perinatal form of HPP or has perinatal HPP without respiratory failure, but is instead diagnosed with HPP later in infancy (infantile hypophosphatasia is diagnosed before 6 months of age while childhood hypophosphatasia is diagnosed after 6 months of age), it is less likely that they will require assistance for breathing but still may require a feeding tube and Strensiq®.
 How can I hold
How can I hold
my baby safely?
Common sense is the best guide for handling a child with HPP. Do not be afraid to show affection to your child by cuddling, rocking, touching and talking to them. Frequent stimulation is necessary for sound emotional and social development. That said, remember that your baby’s bones are soft and fragile, therefore certain precautions need to be considered as outlined in this guide.
 Do I need to give my baby a special diet? Can I nurse?
Do I need to give my baby a special diet? Can I nurse?
Breast milk is an excellent source of calories for virtually all infants, including those with HPP. Babies with all but the most severe forms of HPP should be capable of breastfeeding. However, there are some babies with severe HPP who may have too much calcium in the blood and the urine, and therefore require special infant low-calcium formulas. If the baby is not able to breastfeed, the mother may opt to pump breast milk or formula and feed the child from a bottle, nasogastric tube or G-tube.
 My baby seems to have some gastrointestinal problems
My baby seems to have some gastrointestinal problems
(reflux, upset stomach, constipation) is this linked to HPP?
Reflux is quite common in babies with HPP as is constipation, but they are also quite common in babies without HPP. Generally, therapy that is recommended for babies without HPP is also appropriate for those with HPP, but it is important to talk to your healthcare team about how best to manage any gastrointestinal issues.
 How will this affect
How will this affect
my other children?
Having a baby with HPP affects the entire family, as does the arrival of any new baby. Your other children may experience typical jealously once the baby arrives which can be exacerbated by the amount of time that the parents need to spend with the new baby, given the potential for hospital stays, related travel and HPP appointments. However, children can also become incredibly sympathetic individuals by having a sibling with HPP. They can grow to be extremely caring and open-minded by seeing life with a serious rare disease first-hand.

 I found out I have a change in
I found out I have a change in
the HPP gene (ALPL) do I have HPP?
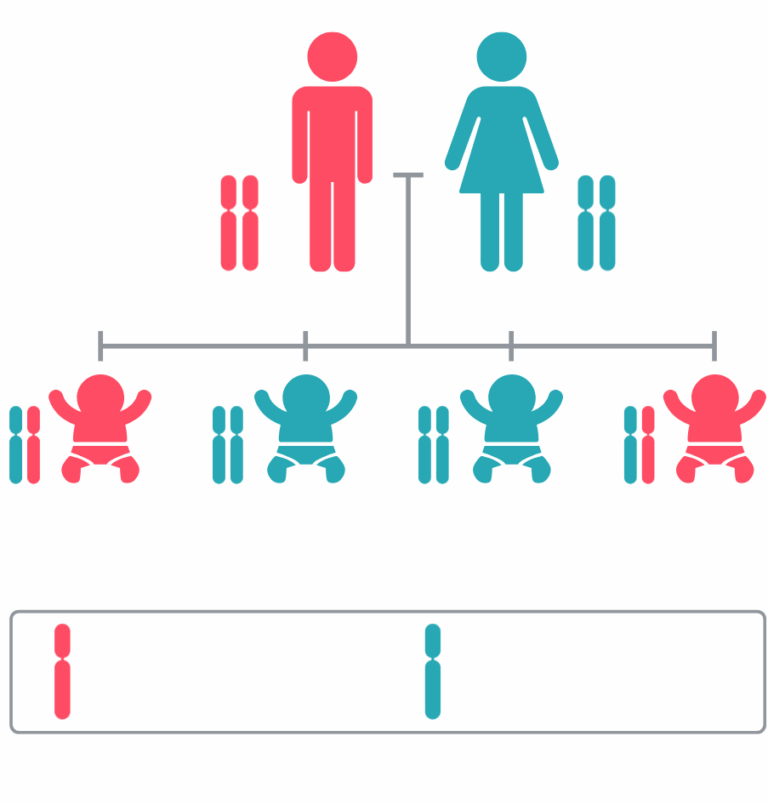
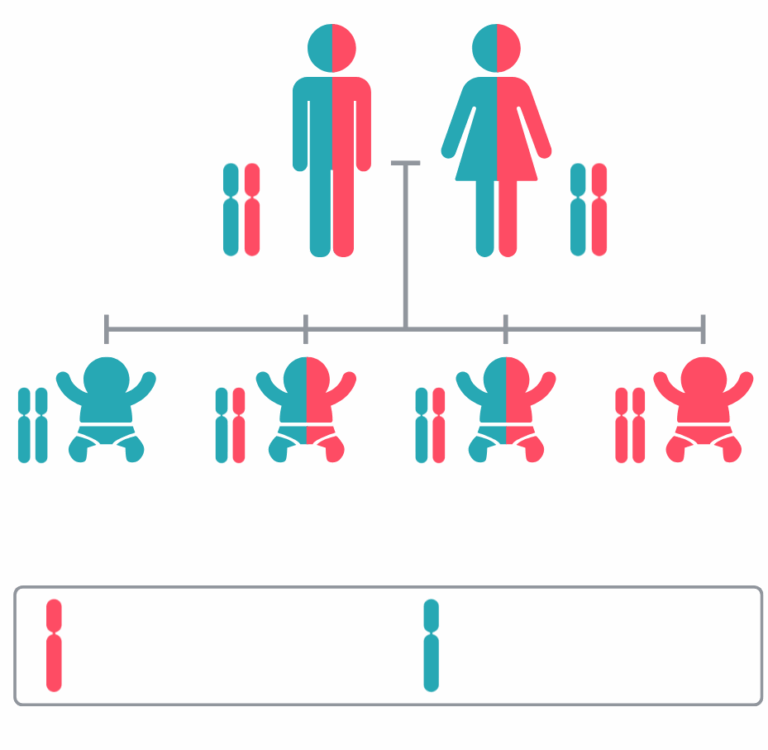
To date, ALPL is the only gene known to be associated with HPP. Typically, with a genetic test, you get either a positive or negative result:
- Positive – this means that the geneticist has found a change in the ALPL gene that causes HPP. Some people with one abnormal copy of the ALPL gene have signs and symptoms of HPP, but almost all patients who present perinatally or in infancy with HPP have changes to both of their copies of ALPL. Other people with a change in one copy of the ALPL gene may not have symptoms of HPP and have traditionally been referred to as “carriers,” although given the complex nature of HPP, that term is not accurate in all circumstances. Whether you have symptoms or not, if you have a change to the ALPL gene, there is a chance you could pass HPP on to your children. Refer to the genetics section of this guide for more information.
- Negative – no change in ALPL was found, meaning you are not a carrier and do not have HPP. On rare occasions there are exceptions to this conclusion as most commercial laboratories cannot analyze 100% of the ALPL gene.
Less common is a result known as a “variant of uncertain significance,” which means that a change in ALPL was found, but the consequences of that change are unknown. Variants of uncertain significance are often part of normal human variation and typically do not cause disease. However, in some cases, due to a lack of currently available data, a particular change in ALPL will be deemed a variant of uncertain significance but will ultimately go on to cause disease. It is important to discuss the nature of any variants of uncertain significance with a genetics professional to understand more.
 I feel overwhelmed, how will I get through this?
I feel overwhelmed, how will I get through this?
First, know that you are not alone on this journey. It is overwhelming to have a child with a rare disease such as HPP. Especially as HPP’s broad range of clinical severity may make it difficult to relate to others’ stories as every journey is so distinct. Support can be found via advocacy organizations (such as Soft Bones), other parents and through your healthcare team. Social media groups can also be useful for support, although it’s important to note that information gleaned from social platforms reflects personal experience or opinions, and it may not be medically accurate or relevant to you. You also have the strongest power of all within yourself – your parental ‘gut’ instinct and love – that will help guide you to make the best decisions for you and your child.
 Pregnancy & Birth Planning
Pregnancy & Birth Planning


 Baby at Home
Baby at Home
 Diet and Nutrition
Diet and Nutrition
As with all children, it is important that children with HPP have a balanced diet that contains enough water, fiber, calcium and vitamin D for their age and size. Breast milk is an excellent source of calories for most infants, including those with HPP. Babies with all but the most severe forms of HPP should be capable of breastfeeding. However, there are some babies with severe HPP who may have too much calcium in the blood and the urine, and therefore require special low-calcium infant formulas. If the baby is not able to breastfeed, the mother may opt to pump breast milk or formula feed the child from a bottle, nasogastric tube or G-tube.

 Teeth
Teeth
Early tooth loss is a clinical hallmark of HPP and for some patients, it may be their only symptom of HPP (odontohypophosphatasia). Regardless of what form of HPP your child has, teeth can fall out at any time for no apparent reason. The enzyme activity of ALP, which is lower than normal in children with HPP, is important for normal tooth development. Lack of (or decreased levels of) ALP activity can result in abnormal formation of the enamel, dentin, and cementum (responsible for anchoring the tooth to the jaw). It is not uncommon for tooth loss to begin between one and two years of age in children with HPP.

 Treatment & Therapy
Treatment & Therapy
 Enzyme replacement therapy
Enzyme replacement therapy
 Physical Therapy
Physical Therapy
 Occupational therapy and safe exercise
Occupational therapy and safe exercise
Healthy Lifestyle

Communicate openly and calmly with children
 Don’t forget to spend special time with children who do not have HPP
Don’t forget to spend special time with children who do not have HPP
Be sensitive to the sibling’s point of view
 Provide guidance about how to safely play with their fragile brother or sister
Provide guidance about how to safely play with their fragile brother or sister
 Teach all children in the family what to do in an emergency
Teach all children in the family what to do in an emergency
Making the Most Of Doctor Visits
 Set a goal
Set a goal
Write it Down
Bring Support
Speak Up
Stay Organized

 Genetics of hypophosphatasia
Genetics of hypophosphatasia
 Your Self-Care
Your Self-Care
 A strong parent can be the best medicine for a child
A strong parent can be the best medicine for a child
 Additional Resources
Additional Resources


